Planning for Positive Change
In each of three previous posts, we looked at Motivational Interviewing (MI) as having four key processes and reviewed practice exercises targeting the first three processes: engaging, focusing and evoking. In this article we examine the fourth MI process: planning.
Commitment language is predictive of behaviour change, and is distinct from preparatory change talk in that it embodies implementation intentions. Consider the following example:
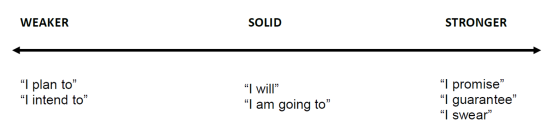
Reference: Miller and Rollnick, 2012: 290
What’s the hurry?
Practitioners often rush toward action planning prematurely, resulting in clients’ reactance and disengagement. Learning to recognize – and strengthen – commitment language signals to us when it is appropriate to move toward the planning process in MI. Also, remember that the four processes are recursive. In other words, even when we hear strong commitment language, clients may still experience ambivalence (evoking process) and decide to re-examine their goals (focusing process). And, as always, we need to continuously engage and re-engage with the other person (engaging process).
Strategies to Strengthen Commitment
Here are some strategies to strengthen clients’ commitment for change:
- Engaging in a supportive and collaborative working relationship
- Focusing on clear goal(s) for change
- Linking the person’s values with their goals
- Evoking the person’s own motivations for change
- Developing a specific change plan
- Determining what step(s) the person is ready, willing and able to take.

We can’t force a plant to grow, but plants are likely to thrive under the right conditions. What about human growth and realizing our potential? Motivational Interviewing provides the “right conditions” in which people can become ready, willing and able to make positive change.
Reflective Practice Questions
Consider a challenging client – one who does not seem to be making progress. Based on your understanding of the four processes of MI (engaging, focusing, evoking, planning), where do you think you need to be with this client? Are there avenues for small, incremental change that you could focus on to evoke commitment language? What might these be?
Come up with a reflection or a question that would evoke commitment language.